
Surgical Management Of Rectal Prolapse Associated With Ileocolic Intussusception And Prophylactic Colopexy In A 2-Month-Old Male Labrador Retriever
Introduction: Intussusception is the telescoping or invagination of one intestinal segment (intussusceptum) into the lumen of an adjacent segment (intussuscipiens). Colopexy is performed to create permanent adhesions between the serosal surfaces of the colon and the abdominal wall so as to prevent caudal movement of the colon and rectum. Colopexy is used most often to prevent the recurrence of rectal prolapse.
Case History and Clinical Examination
A 2-month-old male Labrador retriever puppy named Rocky was presented to the WVS India – ITC clinic with a history of protrusion of mass from the rectum, anorexia, tenesmus, and diarrhea for the last 16 hours. Physical examination confirmed rectal prolapse (Fig. 1). Prolapsed mass was soiled, pink, and hyperaemic.

Abdominal palpation and radiographs revealed an intraabdominal elongated thickened intestinal loop. Ultrasonography revealed multiple hyperechoic and hypoechoic concentric rings in the transverse section which is referred to as the target sign or bull’s eye appearance (Fig 2). A tentative diagnosis of intussusception was made. Differential diagnoses included all other causes of intestinal obstruction (i.e., foreign body, intestinal volvulus or torsion, adhesions, strictures, tumors or congenital malformations).
Clinical parameters on initial physical examination:
Body weight – 3.3 kg Heart rate – 108 bpm Respiratory rate – 28/min Body temperature – 100.1 ℉ CRT – <2 seconds CMM – pink and moist Hydration status – 5% dehydration Peripheral Lymph nodes – NAD
Surgical treatment and Post-operative care:

The puppy fasted for 4 hours. Under general anesthesia, the animal was positioned in the dorsal recumbency, the surgical site was clipped and prepared for aseptic surgery. The prolapsed mass was washed with warm saline to remove the dirt. Ventral midline celiotomy was performed for complete abdominal exploration. Intussusception was found at the ileocolic region (Fig. 3). Ileocolic Intussusception was reduced manually by gently applying traction on the neck of the intussusceptum while milking its apex out of the intussuscipiens. There were no firm serosal adhesions. The affected intestinal segment was examined for viability and perforation.
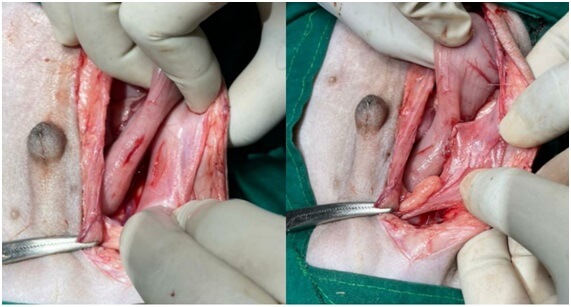
Prolapsed rectal mass was reduced by applying traction on the colon intra-abdominally. The reduction of prolapse was verified by a non-sterile assistant who inspected the anus visually and performed a rectal examination. A 3 cm seromuscular incision was made along the antimesenteric border of the descending colon. A similar incision was made lateral to the linea alba through the peritoneum and the underlying muscle of the left abdominal wall. Edges of the seromuscular incision to the edges of the abdominal wall incision were apposed with two simple continuous rows of sutures using poliglecaprone 25 (Monocryl) 3-0 (Fig. 4). Copious lavage of the peritoneal cavity was performed. The abdominal muscles, subcutaneous tissue was closed in a simple continuous pattern using polyglycolic acid (PGA) 2-0 and the skin with interrupted cross matrix pattern using Polyamide 3-0.
Post-operatively the animal received fluid therapy, systemic antibiotics, and analgesics. The puppy was fed with semi-solid diet and chicken soup. An Elizabethan collar was used to prevent the puppy from biting or licking the surgical site. The puppy recovered uneventfully without any complications (Fig. 5).

Discussion
Intussusception can occur at any age but is most commonly recognized in patients younger than 1 year and therefore should be included among the differential diagnoses for any juvenile patient presented with GI signs. Intussusception most commonly occurs at the ileocecocolic junction but can occur along any portion of the GI tract. Causes of intussusception may include intestinal parasites, viral enteritis, foreign body obstruction, and neoplasia. Previous abdominal surgery is a risk factor.
Diagnostic steps include a complete physical examination, abdominal radiography, and ultrasonography. On physical examination, a thickened tubular or sausage-shaped structure may be palpated in the abdomen. Abdominal radiographs commonly reveal a gas- or fluid-filled bowel consistent with mechanical obstruction. Abdominal ultrasonography is a very helpful diagnostic tool. Multiple hyperechoic and hypoechoic concentric rings in the transverse section (target/ bull’s eye appearance), parallel lines in longitudinal sections, is diagnostic of intestinal intussusception. Colonoscopy can also be used to diagnose ileocolic or cecocolic intussusception.
Treatment of intussusception involves laparotomy with a manual reduction if the affected segment appears potentially viable and/or resection and anastomosis of the intestinal segment if neoplasia is the underlying cause or if the affected segment is necrotic. Arterial pulsations in the mesenteric arteries that are feeding the affected areas, tissue color, wall texture, and peristalsis are some of the most reliable criteria for assessing intestinal viability. Animals with untreated intestinal intussusceptions may die within 3 or 4 days or may live for several weeks. However, for most idiopathic cases of intussusception, the long-term prognosis is good with appropriate aftercare and treatment. Those that die acutely usually have obstructions or enterotoxemia. Prognosis worsens with perforation of the intestine and peritonitis. Death is due to hypovolemia, electrolyte, and acid-base imbalances.
Colopexy is rewarding in preventing the recurrence of prolapse of the rectum. In this case, the colopexy didn’t affect the intestinal function adversely. In cases of the rectal tissue having poor viability because the prolapse has lasted for too long, the case should be managed by resection and anastomosis of the affected intestine.
Importance of vaccination and deworming to prevent Gastro-Intestinal (GI) diseases in puppies
Canine Parvovirus (CPV) is an important pathogen that affects canids worldwide. It mainly affects unvaccinated puppies of 6 weeks to 2 years of age. It causes severe hemorrhagic gastroenteritis and clinical signs include vomiting, hemorrhagic diarrhea, dehydration. It also reduces white blood cell count and the mortality rate in untreated puppies is as high as 70%. Acute intussusceptions must be considered in puppies with parvoviral enteritis that suddenly become worse or that persist much longer than expected. In particular, a diagnosis of ‘chronic parvoviral enteritis’ is very suggestive of intussusception. In many cases of Canine Distemper (CD), epithelium of the GI tract is affected and animals show GI signs such as vomiting and diarrhea. The recommended vaccination schedule for dogs is given in Table 1.
| Age of the Dog | Vaccine |
| 4-6 weeks | DP (Distemper-Parvo) |
| 8-10 weeks | DHPPiL (Distemper, Hepatitis, Parvo, Parainfluenza, Leptospirosis) |
| 12 weeks | DHPPiL booster Anti-rabies vaccine (ARV) |
GI parasites are common pathogens in companion animals. Hookworms (Ancylostoma spp), Roundworms (Toxocara spp) are extremely common in young animals and lead to distended abdomen, intermittent diarrhea, and thickened intestine. Because intestinal parasitism is also a potential predisposing factor for intussusception, fecal samples can also be collected preoperatively for testing and in this case, the puppy was regularly dewormed and no parasitic ova were found. The recommended deworming schedule for dogs is given in Table 2.
| Age of the Dog | Frequency of Deworming |
| Up to 3 months of age | Once in 15 days (deworming should be started at 2 weeks of age) |
| 3 to 6 months of age | Once a month |
| Above 6 months | Once in 3 to 6 months |
Conclusion:
Ileocolic intussusception was surgically corrected by manual reduction of the intussusception and prophylactic colopexy was done to prevent the recurrence of the prolapse. The puppy made an uneventful recovery. The surgical experience and preparedness of the WVS ITC team were of paramount importance in the successful outcome of this case.
